Key Takeaways
- Polysomnography monitors multiple physiological parameters simultaneously, unlike basic home tests.
- It is essential for diagnosing complex issues like narcolepsy, REM behavior disorder, and central sleep apnea.
- The process involves an overnight stay in a controlled clinic environment with a certified technician.
- Results provide a detailed map of your NREM and REM sleep cycles to identify specific disruptions.
What Exactly Happens During a Sleep Study?
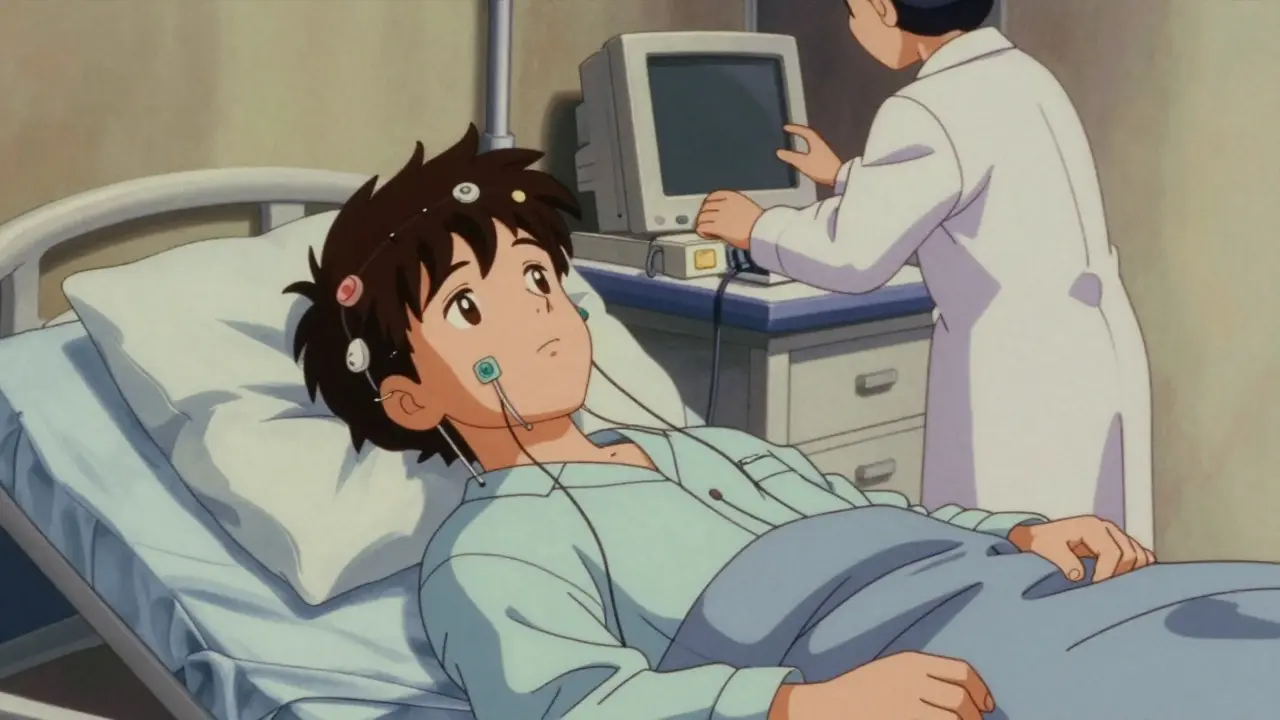
If you've been referred for a sleep study, you aren't just getting a fancy heart monitor. A full polysomnography is a deep dive into your body's nocturnal functions. You'll typically arrive at a sleep center an hour or two before your usual bedtime. A registered sleep technologist will spend about 30 to 45 minutes attaching sensors to your body. Don't worry-while there are often around 22 electrodes and sensors, they are non-invasive.
The goal is to track a variety of data points. For instance, an Electroencephalogram (EEG) tracks your brain waves to determine which stage of sleep you're in. Meanwhile, an Electrooculogram (EOG) monitors your eye movements, which is the primary way technicians identify the REM (Rapid Eye Movement) phase. They'll also use an Electromyogram (EMG) on your chin and legs to see if your muscles are relaxing or if you're twitching and kicking in your sleep.
Beyond the brain and muscles, the test looks at your vitals. Pulse oximetry tracks your blood oxygen levels, while belts around your chest and abdomen monitor your respiratory effort. Airflow sensors under your nose detect if you've stopped breathing or are struggling for air. All of this is recorded alongside your heart rhythm (ECG) and video footage of your movements, giving doctors a holistic view of your night.
Why You Can't Just Do a Home Test
You might wonder why you have to spend a night in a clinic when there are simpler kits you can use at home. The truth is, home sleep apnea tests are a bit like taking a snapshot, whereas polysomnography is a full-length movie. Home tests usually only track 3 or 4 things-mostly breathing and oxygen. If you have simple obstructive sleep apnea, that might be enough. But if your issue is more complex, a home test will miss it entirely.
For example, if you have Narcolepsy, your brain might jump straight into REM sleep without going through the necessary NREM stages. A home test can't see that; only an EEG in a lab can. Similarly, a lab study can tell the difference between Obstructive Sleep Apnea (where your airway is blocked but you're still trying to breathe) and Central Sleep Apnea (where your brain simply forgets to tell your muscles to breathe). The difference in these two is huge when it comes to choosing the right treatment.
| Feature | In-Lab Polysomnography | Home Sleep Test |
|---|---|---|
| Parameters Monitored | 7 to 16 (Comprehensive) | 3 to 4 (Limited) |
| Sleep Staging (EEG) | Yes - Full architecture | No |
| Failure Rate | Low (2-5%) | Higher (15-20%) |
| Diagnoses Narcolepsy? | Yes | No |
| Cost | Higher | 30-50% Lower |

Decoding Your Results: What the Doctor Looks For
Once the night is over, you get to go home, but the work is just beginning for your doctor. A single night's sleep generates over 1,000 pages of raw data. A board-certified sleep physician spends several hours scrubbing through this data to find patterns. They aren't just looking for the number of times you stopped breathing; they are looking at the timing and the context.
They will examine your sleep latency-how long it takes you to fall asleep-and your sleep efficiency. If you're spending too much time in light sleep and not enough in deep sleep or REM, you'll wake up feeling exhausted even if you were in bed for eight hours. They also look for "micro-arousals," which are brief awakenings that you don't even remember but that fragment your sleep and leave you groggy.
For those with suspected severe apnea, some clinics use a "split-night" approach. If the first few hours of the test show obvious, severe apnea, the technician will switch gears and start a CPAP titration. This means they'll apply a mask and adjust the air pressure in real-time to find the exact setting that keeps your airway open, saving you from having to come back for a second visit.
Preparing for the Big Night
Sleeping in a strange room with wires attached to your head isn't exactly a luxury hotel experience. To get the most accurate results, you need to keep your routine as normal as possible. Don't decide to go to bed three hours early just because you're nervous, and definitely don't start a new sleep medication the night before unless your doctor told you to.
One of the biggest pitfalls is caffeine. Avoid coffee, soda, or energy drinks after noon on the day of your test. Caffeine can block the signals your doctor needs to see, potentially masking your true sleep architecture. Also, keep your normal wake-up time for a few days leading up to the study so your body's internal clock is synced.
If you're worried about the environment, remember that most sleep labs maintain a temperature between 68-72°F (20-22°C) to mimic a comfortable bedroom. While some people find it hard to drift off initially, about 85% of patients manage to get enough quality sleep for a valid diagnosis. If you're feeling anxious, just talk to your technician-they're trained to help you relax during the setup.
Alternative Tests and When They're Used
Polysomnography isn't the only tool in the box. Depending on your symptoms, your doctor might order a Multiple Sleep Latency Test (MSLT). This isn't an overnight stay; instead, you take 4 or 5 scheduled naps during the day. This test specifically measures how quickly you fall asleep, which is the primary way to diagnose narcolepsy.
Then there's the CPAP titration mentioned earlier. While often part of a split-night study, it can be a standalone test for people who already have a diagnosis but need their pressure settings adjusted. Because medical technology is moving fast, some clinics are now using wireless sensors to reduce the number of wires from 20 down to just a few, making the experience much less restrictive.
Does a sleep study hurt?
Not at all. Polysomnography is non-invasive. The sensors are placed on the surface of your skin using adhesive pads or straps. There are no needles involved in the standard recording process, though you might feel a bit cluttered with the wires.
Will insurance pay for a sleep study?
Generally, yes, if it's medically necessary. Medicare often covers about 80% of the costs if you meet specific clinical criteria, such as documented snoring, witnessed apnea, or excessive daytime sleepiness. Private insurance usually requires a prior authorization from your doctor.
How long does it take to get the results?
It takes longer than a standard blood test. Because a physician has to manually review hundreds of pages of data, it typically takes a few days to a couple of weeks to generate the final diagnostic report.
What if I can't sleep during the test?
This is a common concern. Technicians are experienced in helping patients settle in. While some people may need a second night to adjust to the environment, the majority of patients get enough sleep to provide a usable diagnostic result.
Is a sleep study the same as a home apnea test?
No. A home test is a simplified version that mostly monitors breathing. A full polysomnography includes EEG (brain wave) monitoring, which allows doctors to see your sleep stages and diagnose non-respiratory disorders like narcolepsy or parasomnias.
Next Steps After Your Study
Once your results are in, your journey toward better sleep actually begins. If you're diagnosed with obstructive sleep apnea, your doctor will likely discuss a CPAP machine or a custom oral appliance. If the study reveals a behavioral issue, like REM sleep behavior disorder (where you act out your dreams), you might be referred to a neurologist for medication management.
If your results come back "normal" but you still feel exhausted, don't give up. Ask your doctor about a Multiple Sleep Latency Test (MSLT) to check for narcolepsy or investigate other factors like iron deficiency, thyroid issues, or chronic stress that can mimic sleep disorders without showing up on a PSG recording.



Srikanth Makineni - 6 April 2026
lab tests way better than home kits
Nathan Kreider - 7 April 2026
I totally get how scary it feels to be wired up like that! Just remember that the technicians are there to help you feel cozy and safe. It really is the best way to get a real answer so you can finally start feeling rested again. You got this!
Brady Davis - 9 April 2026
Oh sure, because nothing says "relaxing night of sleep" like having twenty-two electrodes glued to your face while a stranger watches you snore on a monitor. Absolute luxury. I'm sure the 68-degree room is just a five-star resort experience!
Danielle Kelley - 9 April 2026
Wake up people! Why do they really want those EEG brain wave readings? They aren't just looking for apnea. They're mapping your subconscious for data collection. Why the "controlled environment"? To make sure you don't notice the frequencies they're pumping into the room!
Grace Lottering - 10 April 2026
Data mining while you sleep. Total invasion. Disgusting.
Darius Prorok - 10 April 2026
Actually, home tests are only for simple OSA. If you have central sleep apnea, the home kit is basically useless because it can't tell the difference between a blocked airway and a brain signal failure.
GOPESH KUMAR - 12 April 2026
The irony of modern medicine is that we spend thousands of dollars to be told that we are tired because we don't sleep. It is a fascinating cycle of redundancy. Most people just need to stop looking at screens and embrace the void of silence, yet here we are, quantifying the soul's rest with electrodes.
Benjamin cusden - 14 April 2026
It is quite simplistic to assume that a single night captures the totality of one's sleep architecture. Many of us suffer from the first-night effect, where the novelty of the laboratory setting induces a state of hyper-arousal, thereby skewing the latency data. A truly rigorous diagnostic process would require multiple nights to establish a baseline, though I suppose the insurance companies find that too expensive for the average patient.
Windy Phillips - 15 April 2026
It is truly unfortunate that some people find this process intimidating... perhaps if they had more inner peace, the wires wouldn't be an issue!!! But alas, we must deal with the clumsy realities of the physical form...
Victoria Gregory - 16 April 2026
I think it's so cool how science can actually see our dreams happening through those eye movements!! 🤩 It just shows how connected our minds and bodies are... truly magical in a way!!! ✨💖
Laurie Iten - 16 April 2026
the body has its own wisdom and sometimes the machines just confirm what we already feel in our bones but we keep searching for a number to validate our exhaustion
Kathleen Painter - 18 April 2026
For anyone feeling nervous, just remember that the technicians have seen everything from sleep-walking to extreme snoring, so there is absolutely no reason to feel embarrassed. I've always found that if you bring your own pillow from home, it helps bridge that gap between the clinical feeling of the lab and the comfort of your own bed, which can really help you drift off faster and give the doctors better data to work with in the long run. Just take it one step at a time and focus on the goal of waking up refreshed!
Rauf Ronald - 19 April 2026
Great breakdown of the process! If you're heading in for a study, definitely double-check your insurance's prior authorization requirements so you don't get hit with a surprise bill. Also, if you have a split-night study, the CPAP titration is a total game-changer because it saves you an entire extra trip to the clinic!
Dhriti Chhabra - 20 April 2026
I believe it is most beneficial to approach these medical procedures with a sense of tranquility and trust in the professional staff. While the environment is certainly clinical, the potential for a life-changing diagnosis far outweighs the temporary discomfort of the sensors.
shelley wales - 22 April 2026
It is so important to be patient with yourself during this process. If you can't sleep the first night, please don't be hard on yourself; it's a very common reaction to a new environment and the medical team is trained to support you through that.