Language Access Checker
Why Language Access in Pharmacies Isn’t Optional - It’s a Safety Issue
If you or someone you love takes medication but doesn’t speak English well, getting clear instructions from the pharmacist isn’t a luxury - it’s a matter of life or death. A 2018 study found that nearly one in three adverse drug events among non-English speakers happened because they didn’t understand how to take their medicine. That’s not a mistake. That’s a system failure. And in places like New York, it’s now illegal.
Since 2024, federal law under Section 1557 of the Affordable Care Act requires every pharmacy that takes Medicare, Medicaid, or any federal funding to provide meaningful access to patients who don’t speak English. That means real, professional interpretation - not a family member translating on the spot, not a Google Translate app, not a pharmacy worker who took a Spanish class in high school. This isn’t about being polite. It’s about preventing overdoses, dangerous drug interactions, and people skipping meds because they’re too scared to ask what the pill is for.
What Exactly Are Your Rights as a Patient?
If you’re Limited English Proficient (LEP), you have specific, enforceable rights when picking up prescriptions:
- You are entitled to free, in-person or remote interpretation services at the time you receive your medication.
- Pharmacies must translate key written materials: prescription labels, warning labels like “May cause drowsiness,” and safety instructions.
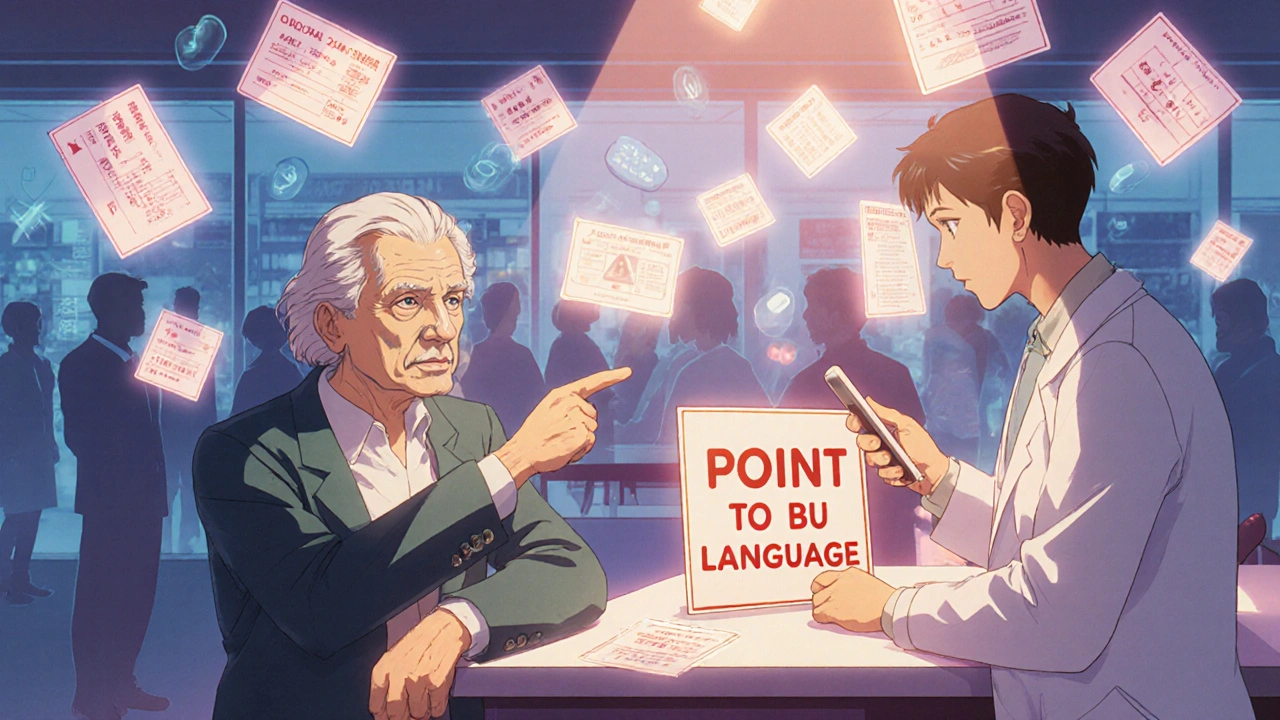
- They must display clear signage near the counter that says “Point to your language” - with pictures of common languages spoken in the area.
- You cannot be forced to use a child, friend, or family member as an interpreter unless you specifically ask for it.
- Interpretation must be available 24/7 for emergency situations, even on weekends or holidays.
These aren’t suggestions. They’re rules. And they’re backed by law - with fines and enforcement actions for violations. In 2022, New York’s Attorney General’s office issued 147 penalties to pharmacies for failing to meet these standards. The most common violations? Missing signs and not offering help when a patient looked confused.
How Do Pharmacies Actually Provide Interpretation?
You might walk into a pharmacy and not see an interpreter sitting at the counter. That doesn’t mean they’re not available. Most pharmacies now use phone or video interpretation services - often through companies like LanguageLine Solutions or TransPerfect. The pharmacist just needs to press a button, and within seconds, a certified medical interpreter appears on a screen or over the phone.
Chain pharmacies like CVS and Walgreens have trained their staff on this. In 2023, they rolled out mandatory 10-hour training modules covering:
- How to recognize when a patient needs help
- How to activate the interpreter system
- What medical terms interpreters must know (e.g., “take with food,” “do not crush,” “avoid alcohol”)
- How to document the service in the patient’s record
Independent pharmacies struggle more. About 33% of small pharmacies in New York still don’t fully comply, mostly because they can’t afford the monthly subscription fees for interpretation services. That’s why the state offers free compliance help through the Office of Language Access Services - but many owners don’t know it exists.

What Languages Are Covered?
It’s not every language under the sun. Federal and state rules say pharmacies must provide services in any language spoken by 1% or more of the local population. In New York City, that means Spanish, Chinese (Mandarin and Cantonese), Bengali, Russian, Arabic, Haitian Creole, and Korean - among others. Each pharmacy must post a list of the languages they support, based on the latest U.S. Census data.
But here’s the catch: Demographics change fast. A neighborhood that had mostly Spanish speakers in 2020 might now have a growing Somali or Urdu-speaking population. The current rules cap services at seven languages per pharmacy, which means some newer immigrant groups still fall through the cracks. Advocates are pushing for updates based on the 2020 Census, expected in early 2025.
Real Stories: What Patients Are Saying
On Reddit, a pharmacist in the Bronx shared: “Since we started using professional interpreters, we’ve had zero medication errors tied to language. That’s not luck - that’s policy working.”
On Yelp, customers praise pharmacies where pharmacists speak their language. One Spanish-speaking patient wrote: “Finally, someone told me why I shouldn’t drink grapefruit juice with my blood pressure pill. No guessing. No fear.”
But complaints still happen. A Chinese patient at a CVS in Queens wrote: “They had the sign. But when I pointed to it, the pharmacist just shrugged and said, ‘We don’t have anyone who speaks Chinese.’” That’s a violation. If they have the sign, they must have the service - even if it’s over the phone.
A 2023 survey by the Asian American Federation found that 68% of LEP patients felt more confident taking their meds after language access improved. But 29% still had trouble getting help on weekends. That’s the gap between policy and practice.
What About the Pharmacies? Are They Overburdened?
Some pharmacists say the rules are too strict. Dr. John Prince of the National Community Pharmacists Association argues that forcing every pharmacy to support seven languages doesn’t make sense in areas with small, scattered populations. He’s not wrong - small shops in rural areas or neighborhoods with only a few non-English speakers shouldn’t have to spend thousands on services they barely use.
That’s why New York allows a one-year waiver if a pharmacy can prove they’re trying but can’t find an interpreter nearby. But they still have to document their efforts and show they’re working to fix it. And even then, they can’t refuse service. If someone walks in needing help, they must find a way - even if it means calling a hotline from the back room.
The real issue? Cost. Training, software, contracts - it adds up. But the cost of not doing it is higher. A 2024 Congressional Budget Office report estimated that these rules prevent about 14,000 emergency room visits each year among LEP patients. That saves $187 million in avoidable healthcare costs. When you look at it that way, interpretation isn’t an expense - it’s an investment in safety.

What’s Changing in 2025?
Things are moving fast. The FDA is working on standardized pictograms for medication labels - simple icons that show “take daily,” “avoid sunlight,” or “shake well.” These will help even if the interpreter isn’t available right away.
California passed similar laws in 2022. Massachusetts is considering one in 2024. And by June 2025, every pharmacy that takes federal funds must have a written language access plan - including staff training records, interpreter contracts, and patient language preference logs.
Some pharmacies are starting to use AI tools to translate labels in real time. But the rules still require a human to verify the translation for medication instructions. Machines can’t yet understand context like “take on an empty stomach” versus “take after breakfast.” That’s why trained interpreters remain essential.
What Should You Do If You’re Not Getting Help?
If you’ve asked for an interpreter and were ignored, or if your label is still in English while others around you have translations, here’s what to do:
- Ask again - clearly. Say: “I need a professional interpreter. It’s my right under federal law.”
- If they still don’t help, ask for the pharmacy manager or owner.
- Take a photo of the “Point to your language” sign if it’s missing or outdated.
- Call the Language Access Help Desk at 1-800-688-8814. They’ll guide you on how to file a complaint.
- Report the pharmacy to your state’s health department or attorney general’s office. In New York, complaints are tracked and public.
You’re not being difficult. You’re protecting your health. And you’re helping make the system better for everyone else who speaks your language.
What This Means for the Future of Pharmacy Care
Language access isn’t just about words. It’s about dignity. It’s about trust. When a patient understands their medication, they’re more likely to take it right. They’re less likely to end up in the hospital. They’re more likely to believe their care team has their back.
The data shows it works. In New York City, medication label translation jumped from 42% in 2006 to 78% by 2015. Access to phone interpreters went from 38% to 92%. And emergency visits for medication errors among LEP patients dropped by 28% over ten years.
This isn’t perfect. There are still gaps. But the direction is clear: healthcare can’t be safe unless everyone understands it. And that includes the person holding the pill bottle.


Evan Brady - 17 November 2025
Let’s be real - this isn’t just about compliance. It’s about survival. I’ve seen grandparents on insulin misread their doses because the label said ‘take once daily’ and they thought ‘daily’ meant ‘whenever I remember.’ Professional interpreters aren’t a luxury - they’re the difference between a stable chronic condition and an ER visit that costs $12k. Pharmacies that cut corners are gambling with lives. And no, ‘we had a sign’ doesn’t cut it if the interpreter button is broken.
Saket Sharma - 19 November 2025
This is pure socialism in action. Why should MY tax dollars fund Mandarin interpreters for some guy who moved here last year? If you can’t speak English, don’t take prescription meds. Simple. The FDA’s pushing this because they’re scared of lawsuits - not because it’s medically necessary. And now they want pictograms? Next they’ll be printing pills in emoji.
Ram tech - 19 November 2025
lol why even bother? pharmacies are already overloaded. they got 1000 patients a day. now they gotta call some hotline for every non-english person? i mean… cmon. just use google translate. its free. and if you cant read english? maybe dont take meds. lol.
Jenny Lee - 20 November 2025
My abuela finally got her blood pressure meds explained properly last week. She cried. Not because she was sad - because for the first time, she didn’t feel stupid. This matters. More than you think.
Erica Lundy - 21 November 2025
The architecture of healthcare equity is not built upon linguistic convenience, but upon epistemological justice. When a patient is rendered linguistically alienated within a clinical space, the very structure of therapeutic trust collapses. The pharmacological act - the ingestion of a substance predicated on precise temporal, contextual, and physiological understanding - becomes an act of faith, not science. The interpreter, then, is not merely a conduit of words, but a reconstitutor of agency. To deny interpretation is to deny autonomy. And autonomy, in medicine, is the first principle.
Kevin Jones - 21 November 2025
They’re calling this ‘language access’ - but it’s really a bureaucratic power grab. The government doesn’t care about your grandma. They care about control. Every interpreter contract is a new line item in a federal budget that’s already bloated. And now they want AI verification? Please. If you can’t say ‘take with food’ in English, maybe you shouldn’t be in a country where the language is English. This isn’t inclusion - it’s assimilation resistance.
Premanka Goswami - 23 November 2025
EVERYTHING IS A LIE. The ‘1% rule’? Fabricated by the WHO to justify globalist surveillance. The interpreters? CIA assets trained to gather biometric data through medical intake. The pictograms? Microchips disguised as icons. You think they care if you understand your meds? They care if you take them - so they can track your DNA, your sleep, your mood. The pharmacy is the new surveillance station. And you’re handing them your pills… and your identity.
Alexis Paredes Gallego - 23 November 2025
Oh wow, another woke mandate. Next they’ll make pharmacies serve halal insulin and gluten-free antidepressants. And who pays? YOU. The guy who works 60 hours a week. The taxpayer. The American. They don’t care about your cost - they care about making you feel guilty for not speaking 12 languages. Meanwhile, the real crisis? The 80% of English speakers who don’t take their meds because they’re too lazy. But no - let’s fix the non-English speakers. Because that’s easier than fixing Americans.
Shravan Jain - 25 November 2025
Let’s analyze the structural inefficiencies: The 33% non-compliant independent pharmacies represent a systemic failure in regulatory enforcement. The subscription cost of LanguageLine Solutions is $1,200/month - a non-trivial burden for a 2-person operation. Yet, the marginal cost of an adverse drug event is $8,700 per incident (CDC, 2023). The ROI is mathematically positive. The failure lies not in policy, but in implementation. And the state’s free compliance help? Undisbursed due to poor outreach - a classic bureaucratic inertia problem. This is not a language issue. It’s a logistics failure.
Brandon Lowi - 27 November 2025
Who authorized this? Who voted for this? No one! It’s bureaucrats pushing this on us - while our own kids can’t read a prescription bottle because they’re too busy TikTok-ing. We’re becoming a nation of linguistic refugees in our own country. And now we’re paying for it? In my grandfather’s day, you learned English - or you didn’t get the medicine. Simple. No apps. No interpreters. No hand-holding. Just responsibility. This is the death of the American work ethic.
Joshua Casella - 27 November 2025
I’ve trained pharmacy techs in three states. This isn’t about politics - it’s about people. I’ve seen a Somali woman in Minneapolis hold up her insulin vial and whisper, ‘Is this for my daughter?’ - because no one ever asked if she understood. When we activated the interpreter, she sobbed. Not because she was scared - because someone finally listened. This isn’t a cost. It’s a covenant. And if you think that’s too soft for a pharmacy, you’ve never held someone’s life in your hands.
Richard Couron - 29 November 2025
They say ‘meaningful access’ - but what they really mean is ‘forced multiculturalism.’ You think this is about safety? It’s about erasing American culture. Why should a pharmacy in rural Nebraska have to provide Korean interpreters? There’s one Korean family in the whole county! This is cultural colonization under the guise of ‘health equity.’ And don’t tell me it’s ‘federal law’ - the Constitution doesn’t say you have to translate for every immigrant who walks in. This is tyranny dressed in a white coat.
Alex Boozan - 1 December 2025
They’re using AI translation for labels? That’s a disaster waiting to happen. ‘Take on an empty stomach’ becomes ‘consume without food’ - and the patient thinks it means ‘don’t eat anything ever.’ Machines don’t understand context. They don’t know that ‘shake well’ means ‘don’t let the crystals settle’ - they just convert words. And if the interpreter is remote? What if the connection drops? What if the interpreter is unlicensed? What if they’re a bot pretending to be human? This is a security nightmare. And they’re calling it progress?
mithun mohanta - 2 December 2025
Oh, how quaint - the state subsidizes linguistic services while our public schools can’t teach basic grammar. The irony is exquisite. We now require pharmacies to offer Bengali interpreters, yet our own children can’t conjugate verbs. This is not equity - it’s performative virtue signaling. The real crisis? The erosion of linguistic competence in the native population. We’re building multilingual infrastructure while our own citizens are becoming monolingual idiots. The pharmacy is not the problem. The education system is.
steffi walsh - 3 December 2025
This made me cry. Not because it’s sad - because it’s so simple. Someone just needed to be heard. And now, because of this, someone else won’t end up in the hospital. That’s not policy. That’s love. Thank you for writing this.